
By George Weber, President and CEO, The Royal
Earlier this year, I opened a speech at a business breakfast by asking attendees to raise their hands if they knew a colleague, family member or friend who has struggled with mental illness. Every person in the room raised a hand.
Ten years ago, at a similar event shortly after I became CEO of The Royal Ottawa Health Care Group, I asked the same question. Less than a quarter of the audience responded. Many were tentative, casting furtive glances around the room to make sure others were raising their hands, too.
A lot has changed. Mental health and illness has become a conversation that’s alive and well in communities and corporations across Canada. The days are rare when you don’t read or hear about mental health in the news. For many, it’s a frequent topic of conversation with family, friends, and even coworkers.
In the last 10 years, many reports on how to address mental illness have crossed my desk. I’ve seen countless calls to action. We have the evidence. Where’s the action?
In 2006, mental health saw a boost in public exposure with the release of Senator Michael Kirby’s forward-looking report, Out of the Shadows at Last: Transforming Mental Health, Mental Illness and Addiction Services in Canada.
That report gave voice to the millions of Canadians living with mental illness and addictions, as well as their caregivers, in a way that was difficult to ignore. It laid the foundation for creating the Mental Health Commission of Canada in 2007. Since then, that commission has done great work to bring people and organizations together to strategize improving mental health across Canada.
In 2012, the Mental Health Commission of Canada published Changing Directions, Changing Lives: The Mental Health Strategy for Canada. The commission’s leadership wrote that “We can and must defeat the stigma that has blighted people’s attitudes for far too long and has fed the discrimination that so many have endured.”
The strategy recommended mental health promotion for people of all ages, in all places; better access to care; reduced disparities of mental illness risk factors; better mental health care for Indigenous Canadians; and the need for government at all levels to unite in a comprehensive approach to mental health system transformation.
This publication has been influential, and in the years since Canada has taken great strides toward the goal of stigma reduction. More Canadians are willing to speak openly about mental health than at any point in living memory. As for the other goals, we haven’t succeeded yet.
Back in 2002, Roy Romanow’s report on the future of health care in Canada noted that, “We must transform our health care ‘system’ from one in which a multitude of participants, working in silos, focus primarily on managing illness, to one in which they work collaboratively to deliver a seamless, integrated array of services to Canadians, from prevention and promotion to primary care, to hospital, community, mental health, home and end-of-life care.”
Are we there yet? No, and in mental health — what Romanow called health care’s “orphan child”— we have barely budged. In any given year, one in five Canadians experiences a mental health issue, with a cost to the economy well in excess of $50 billion. One in three Canadians will experience a mental health problem in their lifetime.
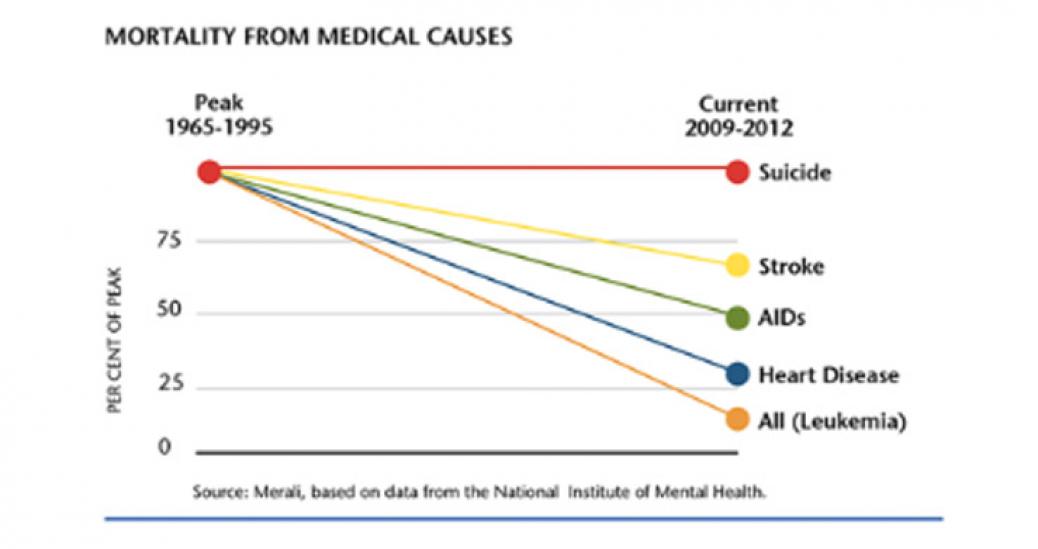
"Most of all, we need an integrated approach that is prevention-oriented, attuned and responsive to social determinants of health, and equity-focussed - especially when it comes to Canada's most vulnerable populations."Despite advances in treatment, Canada’s suicide rate hasn’t moved. According to the National Institute of Mental Health, the United States has seen mortality rates from stroke, AIDS, and heart disease drop significantly from their peaks in the last 50 years — the statistics are similar for Canada. When will we be able to say the same for suicide?
The Royal, alongside the Mental Health Commission of Canada and the Canadian Alliance on Mental Illness and Mental Health, has advocated for a national suicide prevention strategy backed with both funding and a mechanism for action. This call has garnered much support, but has yet to result in a financial commitment.
The $5 billion over 10 years in mental health funding tied to last year’s Health Accord is a good start, but mental health funding needs to be seen as a marathon, not a 50-metre dash. Mental health service providers such as The Royal have seen a building tsunami of people seeking help. The Royal and its peers have also had minimal funding increases for mental health treatment over the last seven years. We’ve seen a lot of announcements, but there’s a chasm between words and change that actually affects the frontlines of mental health care.
We need to move faster. We’ve been crushing stigma, and successes there mean more people are seeking the mental health care they need. The challenge is to find the resources, coupled with research and standardization, to keep pace with increasing demands.
Those living with mental illness, and those supporting them, are being underserved by a fragmented system that is incapable of responding to their spectrum of needs. We need unified effort from government on all levels to change this, and the funding to back it up.
Recently, Dr. David Clark, Britain’s leading expert in Cognitive Behavioural Therapy and an innovator in making publicly funded, evidence-based psychotherapy widely available, visited The Royal and shared the keys to success for the Improving Access to Psychological Therapies (IAPT) program in England. His work demonstrates the potential positive outcomes of a nationally implemented, standardized access-to-care strategy.
IAPT makes evidence-based psychological treatments for depression and anxiety disorders available in every community in England. It has also demonstrated that the initial investment to establish access to structured psychotherapy can in fact offer a significant return on investment through reduced physical health care costs, savings on benefits and taxes, and increased GDP. In the last year, a number of provinces have made tentative steps to expand access to structured psychotherapy. As this moves forward, we should not forget the hard lessons and experiences that have led to IAPT’s success.
The growth we’ve seen in public dialogue has happened in large part because of the generosity of those living with mental illness and their caregivers, who have taken the time and done the hard work of sharing their stories and advocating for change.
At The Royal’s annual Inspiration Awards Gala, we honour mental health advocates. This year, one of our awards went to Pat Capponi for her work channelling her lived experience into real change.
“We have learned together, banded together, not in denial of mental illness, but in determination to raise our voices, and our expectations of ourselves and of the system,” Capponi said.
These people are the guides to creating a better system, but the burden of systemic change should not be on them alone. If the conversation we’re now having about mental health has shown anything, it’s that mental illness touches everyone.
Inextricably linked to health care, and especially mental health care, is research. The Royal is a mental health care, research, and teaching hospital, and scientists at our Institute of Mental Health Research work with the goal of research informing practice, and care driving research. There’s a crucial link between research and applied health system innovation — from bench to bedside.
Only 4.3 per cent of annual health research spending in Canada goes to mental health research, according to an analysis by Dr. Zul Merali, President and CEO of The Royal’s Institute of Mental Health Research. Another 1.4 per cent of health research spending goes to substance use research.
Mental illness accounts for a massive burden of disease —at least 1.23 times that of cancer, and more than 1.5 times if we include addictions. If we funded mental health research at 1.23 times the amount we spend on cancer research, we would be allocating $667 million annually. That would be $577 million more funding than mental health research currently receives.
Research is one of the biggest keys to improving mental health care longer-term. There are so many unanswered questions about our brains and mental health, and with answers comes the potential for transformative discoveries that will bring hope to many suffering in Canada and around the world. Why aren’t we backing these research questions with money?
We may need to get more creative in how we allocate research dollars in order to invest in the work with the highest potential return on investment. In this moment, it is critical that we empower clinical research that will lead to better diagnosis and personalized treatment. We need to put new, better tools in the hands of our care providers in order to face the enormous demand for mental health care now and in the future.
"There are so many unanswered questions about our brains and mental health, and with answers comes the potential for transformative discoveries that will bring hope to many suffering in Canada and around the world. Why aren't we backing these research questions with money?"Let me be clear: I am an optimist and can see a brighter future, but I’m also a realist. We have made much progress in the last 10 years in terms of raising awareness and decreasing stigma surrounding mental health. That is a legacy in which I’ve been proud to play a role.
Alongside this progress, however, we need more action and less ink. We need a long-term, more significant, continuous federal investment in mental health — including dedicated research funding. We need robust research collaboration, a cohesive and holistic approach to health, new treatment modalities that include early intervention, intergovernmental coordination on an unprecedented level, and funding for increased frontline capacity.
And, most of all, we need an integrated approach that is prevention-oriented, attuned and responsive to social determinants of health, and equity-focussed — especially when it comes to Canada’s most vulnerable populations.
As CEO of The Royal, I’ve seen the massive cultural shift surrounding mental health. It’s exciting, but it’s releasing a deluge of demand for mental health care. I hope this flood will create fertile ground for a new era in which we focus on building not only personalized interventions, but also mental resilience, equity, and a strong support system that is there when people need it most.